In pain? – Let us help you
Pain is the most common reason for anyone making an appointment in our clinic. Pain comes in many forms, sharp, dull, a feeling like brusing, and how you describe it to us is important to understanding the cause.
Below are some of the areas oif the foot that commonly ‘hurt’ but the list isn’t exhaustive and sometimes more than one area is involved.
Toes and nails
Our nails tend to grow more slowly and more thickly as we get older. This is often a result of reduced circulation and years of bashing them against the inside of the end of shoes which make them thicken.
The function of a nail is to protect the end of a toe. Trauma or repeat stress stimulates the body’s protective mechanism making the nails thicker so they offer more protection. This increases the pressure on the end of the toe and can make them sore, even painful, and the nails harder to cut.
One person in 50 will develop this condition called onychogryphosis. A thickened nail – unsightly and painful when pressing against the inside of a shoe.
This can occur at any age but is more likely as we get older and anyone with onychogryphosis can benefit from visiting a Podiatrist.
Thickened nails often need to be reduced and shaped with an electric file before they can be cut. This reduces discomfort, pain, pressure and maintains the foot in better condition and prevents it from getting worse.
Joint pain?
One person in six over 50 will develop osteoarthritis in the mid-foot. According to a recent study at Keele University’s Arthritis Research UK Primary Care Centre. Osteoarthritis is characterised by inflammation around the joints, damage to cartilage and swelling, which causes pain, stiffness and restricts movement. Sometimes it causes bony bumps on the top of the foot and it is possible to develop osteoarthritis just in the feet.
The foot comprises 26 bones, 12 of which are in the mid-section. A big hip joint is well designed to take the whole body weight but that same weight has to go through each individual bone and small joint in the mid-foot. Risk factors include genetic predisposition, injury to the area and overuse.
Runners and people who stand for a living are more likely to develop problems. Good trainer-type shoes will help to minimise stress and ease pressure on joints as well as judicious use of the right orthotic insoles.
What can your Podiatrist do for arthritic foot pain?
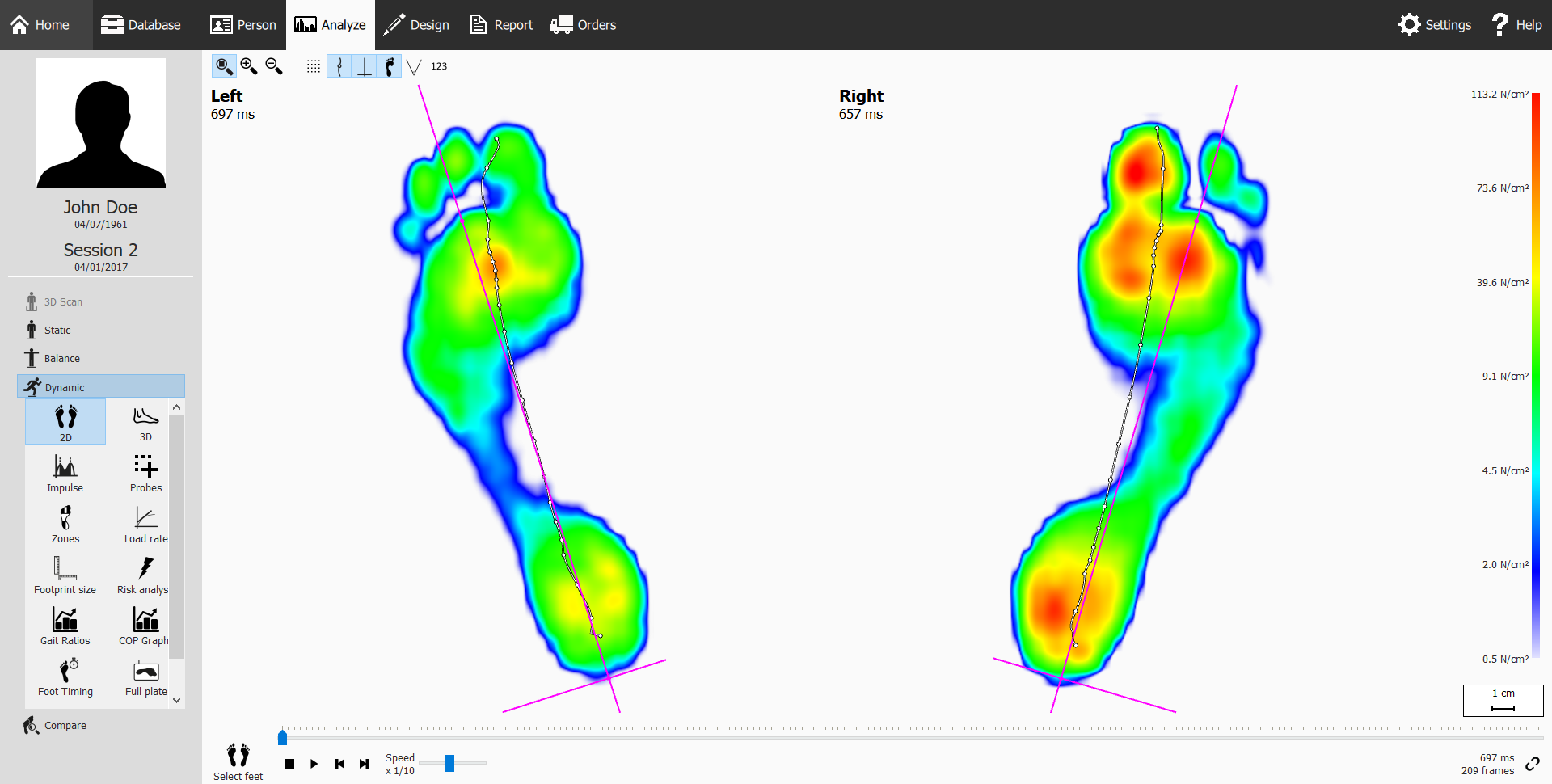
Advice starts with evaluation. This comprises consultation, palpation, range of motion checks, leg length measurement and gait assessment with Footscan. From this you might have general advice, exercise recommendations, insoles and ultimately omward referral to an orthopedic consultant.
If you have any foot pain, see one of our Podiatrists for consultation, examination, assessment, report and discussion of findings and development of a treatment plan.
Corns or verrucas?
Commonly found over a joint surface, between the toes or on the sole of the foot, corns are a common cause of pain. They are usually caused by pressure and friction. Corns are areas of callous with a hard central portion that focuses pressure on the underlying structure and can cause momentary, sharp, eye-watering pain when compressed. They are formed of dead skin and have no blood supply.
A verruca is different because it is a viral infection of the skin and has a blood supply. Verrucas can also cause pain because they are also rich in nerve tissue. This means that when they are compressed – they hurt!
Your Podiatrist can remove your corn completely but if the pressure and friction remain, they will grow back in time. Shoes are a common cause of corns and a change of footwear type can bring relief. Appropriate padding can also help.
Verrucas present a different problem and some treatment options can be found here.
What else could be causing my foot pain and what other treatments are available?
There are other possibilities including trauma, bruising, Morton’s neuroma, muscle damage or overusen or a foreign body such as a piece of glass or an embedded hair.
Consultation is the start point, but for both chronic (experienced over a long period) or acute (recent or rapid onset) pain, we have a number of options including laser and Shockwave.
If you would like more information, or to make an appointment with one of our Podiatrists, call Maidenhead Podiatry on 01628 773588 or e-mail info@maidenheadpodiatry.co.uk.